Learn more about abnormalities of the auricle’s orientation.
Abnormalities of the auricle’s orientation
Author: Ian Suchet1, Janelle Santos2
1. Ian Suchet MBBCh FRCPC, Calgary MFM Centre, EFW Radiology, Calgary, Alberta Canada
2. Mayo Clinic, Department of Obstetrics and Gynecology, Rochester, MN, USA
Reviewers: Karen Fung-Kee-Fung, Mauro Schenone
View the Patient Information leaflet
Orientation of the auricle
a. Normal orientation of the auricle (Figure 8).
b. Posteriorly rotated ear. Defined as an ear that is posteriorly rotated along it’s longitudinal-vertical axis and usually appears low. When this rotation is extreme, and the longitudinal axis is parallel to the body of the mandible it is called melotia.
The etiology and pathogenesis of posteriorly rotated ears as a variation and malformation are unknown. It has been perceived as a developmental arrest; that is, the external ear, which normally is situated in some degree parallel to the developing mandible, does not rotate properly to the side of the face. The actual frequency of posteriorly rotated ears is unknown, but, if one uses the percentiles in Farkas (1) curve, 2% of people would fall below the curve by definition alone. Mild degrees of posterior angulation are very nonspecific and common and are not particularly useful in the recognition of syndromes.
Ultrasound
Once the volume is acquired, the 3D rendered image is rotated to a sagittal plane to enable visualization of the profile of the head and face. The render box is widened to allow the entire face and auricle to be visible in the same image.
Subjective assessment of ear rotation is unacceptable because it is unreliable and often confounded by changes in head position.
Two techniques are described to measure ear rotation:
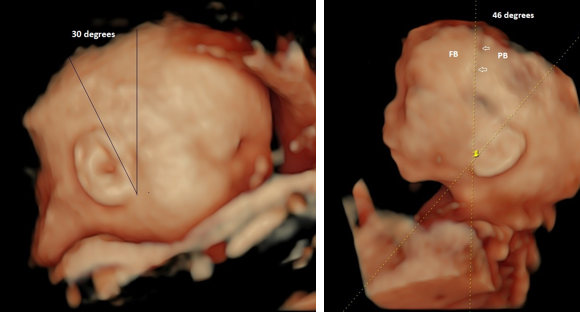
- The diagnosis is made when the angle formed by the line perpendicular to the Frankfurt horizontal - plane and the medial longitudinal axis of the ear (the two most remote points of the ear) is greater than 20 degrees (Figure 31 a). This angulation is measured by establishing the Frankfurt horizontal (FH), dropping a perpendicular line onto the FH at the ear, and measuring the angulation away from the vertical. Range of normal in school-aged children is usually between 10° and 20°. The Frankfurt plane is a horizontal plane extending through the lateral profile of the face with the head in a neutral position. The imaginary line is drawn from the EAM to the area just under the eye (infraorbital rim) and should be parallel to the ground.
- The auricle is measured from the helix to the lobe and a first line drawn through these two points creates the vertical plane of the auricle. A second line was drawn from the top of the head, running parallel between the frontal and parietal bone through the coronal suture. The intersection of these two lines creates the rotational angle of the ear (Figure 31 b). In the study by Ginsberg et. al. (2) the median ear angle was 7.5 degrees in Euploid fetuses. A value of 28 degrees or greater was chosen as the ‘cut-off’ for ear rotational abnormality as this was the lowest value that included all fetuses with chromosome abnormalities. An abnormal ear rotation was also observed among nine fetuses with normal chromosome complements, resulting in a false positive rate of 3%.
Problem: Abnormalities of ear shape may make it difficult to reliably determine the medial longitudinal axis of the ear. In such cases, it is probably unwise to assess the rotational status of the ear.
Associated anomalies
Posterior rotated ears may be present in several chromosomal anomalies but are most common in Turner syndrome and Noonan syndrome.
References
- Farkas I.G: Anthropometry of the Head and Face. Raven Press, New York, 1994.
Ginsberg NA, Cohen L, Duncan JS et.al. 3-D ultrasound of the fetal ear and fetal autosomal trisomies: a pilot study of a new screening protocol. Prenat Diagn 2011; 31: 311–314
Figure 31. Posterior rotation of the ears.
a. 30 degrees.
b. 46 degrees.
Both auricles appear falsely low set (due to the posterior rotation of the auricle) based on the relationship between the auricle and outer canthus of the eye.
FB frontal bone; PB parietal bone; open arrows coronal suture.
Auricular Protrusion
Auricular Protrusion / Protuberant – Prominent ear
A protuberant / protruding ear is a laterally prominent auricle that stands out from the head at an increased angle. The ear is generally normal in size.
Smith and Takashima (1) described the protruding ear as a result of a developmental defect in the posterior auricular muscle. One role of the posterior auricular muscle is to draw the pinna towards the skull, and dysfunction of this muscle causes the pinna to protrude. According to the author, the protruding pinna should be considered a part of the neuromuscular defect and not articular cartilage dysmorphogenesis. There is usually underdevelopment of antihelical fold (which is flattened) and overdevelopment of the concha causing the helix to protrude (2). The normal angle between the scapha cartilage and concha cartilage increases from about 90 degrees to 130 degrees (3).
In a Japanese study, protruding ears was recognized as an acquired defect as the frequency in the newborn period was 1% and the frequency at 1 yr of age was 5.5 % (4).
Etiology
- Usually idiopathic / normal variant.
- May be associated with syndromes.
- Syndromes / disorders in which protruding auricles occur as a feature include:
- Aarskog syndrome (hypotelorism, shawl scrotum, short stature).
- Myotonic dystrophy.
- Anencephaly.
- Cohen syndrome (distinctive face/teeth, long thin fingers).
- Tricho-rhino-phalangeal syndrome (sparse hair, prominent nose, brachydactyly, short stature).
- Noonan syndrome.
- Coffin-Lowry syndrome (course face, tapered fingers, pectus carinatum).
- Mandibular – facial dysostosis (Toriello type).
- Kabuki syndrome (distinctive face, long palpebral fissures, short stature and mental retardation).
- Langer‐ Giedion syndrome
- Congenital muscular dystrophy anencephaly,
- Trisomy 21
- Trisomy 18
- Trisomy 8
- 18 p syndrome
- Del 4p
- Turner syndrome.
Ultrasound
Diagnosis
Two techniques are reported:
- The most used method to assess protrusion is to measure the gap between the rim of the helix and a point on the mastoid perpendicular to the helix rim. The diagnosis is made if the outer edge of the helix is more than 2 cm from the mastoid at the point of maximum distance (Figure 32 a). The disadvantage of this method is that any variation in shape or position of the mastoid can influence the measurement. Driessen et al (5) found a sex difference between males and females.
- The second method of assessment is the angle formed by the plane of the ear and the mastoid – occipital bone (auriculocephalic angle, Figure 32 b). The diagnosis is made if the ear protrudes by > 30-40 degrees from mastoid bone. Measurement is made from the rim of the helix to a point on the mastoid bone perpendicular to the helical rim.
The normal relationship between the auricle and mastoid bone is depicted in figure 8.
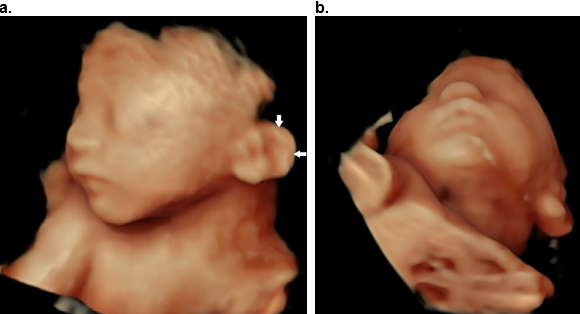
The diagnosis can be made in more severe cases on the frontal oblique views (Figure 33).
Figure 32. Auricular protrusion. 3D surface rendered image in an AP (coronal) plane.
a. There is an increased distance of 2.2 cm between the descending helix of the ear and the mastoid bone.
b. There is an increased auriculocephalic angle (54 degrees).
c. Postnatal image of a normal 4 yr old patient with a protuberant ear (2.3 cm distance between the helix and mastoid bone). With permission.
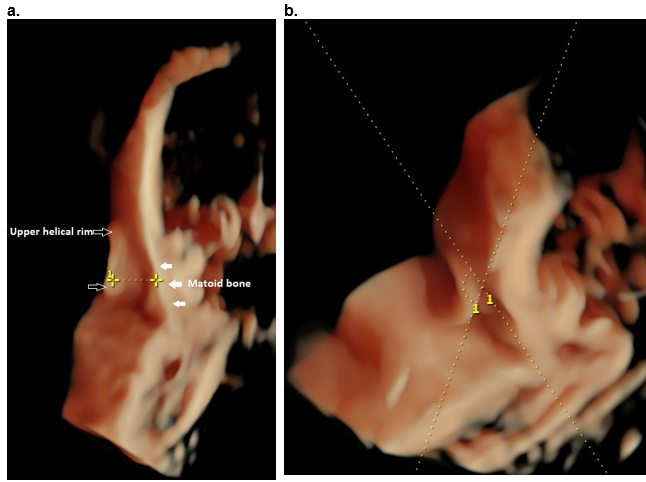
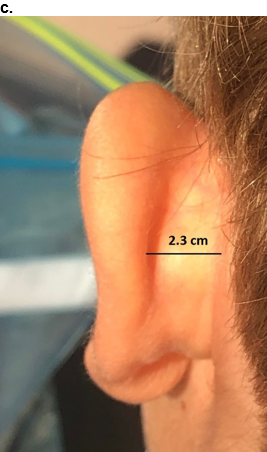
Figure 33. Auricular protrusion on the frontal oblique view.
a,b. Surface rendered view of a protuberant ear (closed arrows, a) in a normal fetus
References
- Smith DW, Takashima H. Protruding auricle: A neuromuscular sign. Lancet, 1978;1(8067): 747–749.
- Carey JC. 1993. External ear: 5.12 Protruding ear. In: Human Malformations and Related Anomalies (eds RE Stevenson, JG Hall, RM Goodman). New York: Oxford University Press.
- Stevenson RE, Hall JG. Human malformations and related anomalies. 2005. 2nd edition. Oxford University Press.
- Matsuo K, Hayashi R Kiyono M et.al. Non surgical correction of auricular deformities. Clin Plast Surg 1990;17:383.
- Driessen JP, Borgstein JA, Vuyk HD. 2011. Defining the protruding ear. J Craniofac Surg 2011;22(6): 2102–2108.
This article should be cited as Suchet I, Santos J: Abnormalities of the auricle’s orientation. Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, www.isuog.org, June 2023.
Leave feedback or submit an image
We rely on your feedback to update and improve VISUOG. Please use the form below to submit any comments or feedback you have on this chapter.
If you have any images that you think would make a good addition to this chapter, please also submit them below - you will be fully credited for all images used.
Feedback form
Please note that the maximum upload size is 5MB, and larger images and video clips can be sent to [email protected].