Learn more about abnormalities of the auricles’s position.
Abnormalities of the auricles’s position
Author: Ian Suchet1, Janelle Santos2
1. Ian Suchet MBBCh FRCPC, Calgary MFM Centre, EFW Radiology, Calgary, Alberta Canada
2. Mayo Clinic, Department of Obstetrics and Gynecology, Rochester, MN, USA
Reviewers: Karen Fung-Kee-Fung, Mauro Schenone
View the Patient Information leaflet
Position of the auricle
1. Normal position of the auricle (see image 2).
2. Melotia – ear located on cheek due to absent ascent.
Melotia is a term used in the older literature to refer to a strikingly posteriorly rotated ear where the actual longitudinal axis of the ear is almost parallel to the body of the mandible and the ear may be situated close to the angle of the mandible on the cheek. This is thought to be due to lack of ascent of the ear.
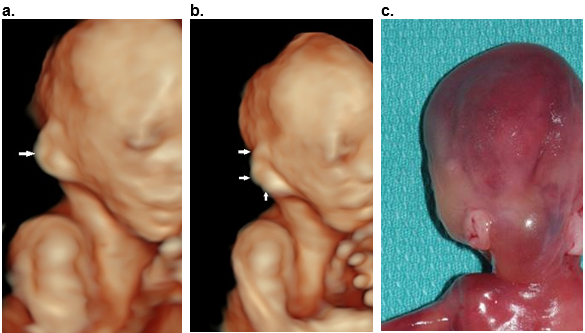
Figure 24. Melotia.
a,b. 3D surface rendered images of the right ear at 21 wks of gestation (arrows). The right ear located on the posterior cheek and enlarged (macrotia).
Postabortal image demonstrates the abnormal location of both ears with microtia of the left ear and macrotia of the right ear.
Otocephaly / Synotia
c. Otocephaly / Synotia: Agnathia Otocephaly Complex also known as agnathia-microstomia-synotia complex, agnathia-holoprosencephaly.
Otocephaly is a severe congenital, lethal defect with an incidence of less than 1 in 70,000 births (1).
Synotia – ears are close to each other or fused in the midline.
Otocephaly may occur alone or in association with other malformations, including holoprosencephaly and heterotaxy.
Otocephaly is a first branchial arch defect believed to result from alteration in neural crest cell migration. A defect in blastogenesis causes the first branchial arch to fail to develop into the lower jawbone, parts of the ear and the anterior two-thirds of the tongue (1).
Pathogenesis/Etiology
Most reported cases occurred sporadic; although a few familial cases are known, indicating a genetic background (1).
Multiple other etiologies can contribute to this pathogenesis.
- Medications such as theophylline, corticosteroids, rufochromomycin, bruneomycin, and trypan blue may increase the risk among pregnancies (2).
- Genetic etiologies include the absence or abnormal expression of the PRRX1 gene (chromosome 1q23) and diminished expression of bone morphogenetic protein 4 and transforming growth factor-beta. The transcriptional factor OTX2 (chromosome 14q23) is also thought to be implicated (2-4). Apart from craniofacial organization, PRRX1 and OTX2 are involved in regulation of central nervous system, eye and limb development.
Ultrasound
Prenatal detection is typically reported during the second and third trimesters, although it may be possible in the first trimester (5).
- This condition represents the most extreme form of auricular malposition. The malformed auricles are located in an anterior, caudal and more horizontal position near the midline. In the most severe form the auricles appear on the face. The abnormal auricles are in the usual position of the mandible (melotia) or even auricular fusion (synotia) may be present. The ventral position of the ears differentiates the anomaly from other syndromic pathologies such as Treacher Collins syndrome, Goldenhar, Pierre Robin sequence or Nager syndrome (5).
- There is marked hypoplasia or absence of the mandible.
- The mouth is small (microstomia) or absent and the tongue is hypoplastic.
- Polyhydramnios due to impaired swallowing and airway obstruction may be present.
- This condition may occur with other malformations such as holoprosencephaly, ophthalmologic abnormalities, situs inversus or skeletal deformities (6-8).
- Other facial malformations include hypotelorism, cyclopia, unilateral/bilateral microphthalmia/anophthalmia, short and laterally downward-sloping palpebral fissures) and nose (proboscis, large nose) as well as facial clefts possible (1).
Few children have been known to survive the perinatal period and needed extensive reconstructive surgery, aside from tracheostomy and gastrostomy feeding (6).
References
- Vanhees L, Denayer E, Thaens A et.al. Agnathia-otocephaly complex: a case report and literature review on recurrence risk. Care Rep Perinat Med 2020;9(1):20200041.
- Dasouki, M, Andrews, B, Parimi, P, Kamnasaran, D. Recurrent agnathia-otocephaly caused by DNA replication slippage in PRRX1. Am J Med Genet 2013;161:803–8.
- Chassaing, N, Sorrentino, S, Davis, EE, Martin-Coignard, D, Iacovelli, A, Paznekas, W, et al. OTX2 mutations contribute to the otocephaly-dysgnathia complex. J Med Genet 2012;49:373–9.
- Sergouniotis, PI, Urquhart, JE, Williams, SG, Bhaskar, SS, Black, GC, Lovell, SC, et al. Agnathia-otocephaly complex and asymmetric velopharyngeal insufficiency due to an in-frame duplication in OTX2. J Hum Genet 2015;60:199–202.
- Rodrigyez N, Casabuenas A, Andreeva E et.al. First trimester diagnosis of agnathia-otocephaly complex: a series of 4 cases and review of the literature. J Ultrasound Med 2019;38:805-809.
- Gekas, J, Li, B, Kamnasaran, D. Current perspectives on the etiology of agnathia-otocephaly. Eur J Med Genet 2010;53:358–66.
- Donnelly, M, Todd, E, Wheeler, M, Winn, VD, Kamnasaran, D. Prenatal diagnosis and identification of heterozygous frameshift mutation in PRRX1 in an infant with agnathia-otocephaly. Prenat Diagn 2012;32:903–5.
- Sergouniotis, PI, Urquhart, JE, Williams, SG, Bhaskar, SS, Black, GC, Lovell, SC, et al. Agnathia-otocephaly complex and asymmetric velopharyngeal insufficiency due to an in-frame duplication in OTX2. J Hum Genet 2015;60:199–202.
Ultrasound
Prenatal detection is typically reported during the second and third trimesters, although it may be possible in the first trimester (5).
- This condition represents the most extreme form of auricular malposition. The malformed auricles are located in an anterior, caudal and more horizontal position near the midline. In the most severe form the auricles appear on the face. The abnormal auricles are in the usual position of the mandible (melotia) or even auricular fusion (synotia) may be present. The ventral position of the ears differentiates the anomaly from other syndromic pathologies such as Treacher Collins syndrome, Goldenhar, Pierre Robin sequence or Nager syndrome (5).
- There is marked hypoplasia or absence of the mandible.
- The mouth is small (microstomia) or absent and the tongue is hypoplastic.
- Polyhydramnios due to impaired swallowing and airway obstruction may be present.
- This condition may occur with other malformations such as holoprosencephaly, ophthalmologic abnormalities, situs inversus or skeletal deformities (6-8).
- Other facial malformations include hypotelorism, cyclopia, unilateral/bilateral microphthalmia/anophthalmia, short and laterally downward-sloping palpebral fissures) and nose (proboscis, large nose) as well as facial clefts possible (1).
Few children have been known to survive the perinatal period and needed extensive reconstructive surgery, aside from tracheostomy and gastrostomy feeding (6).
References
- Vanhees L, Denayer E, Thaens A et.al. Agnathia-otocephaly complex: a case report and literature review on recurrence risk. Care Rep Perinat Med 2020;9(1):20200041.
- Dasouki, M, Andrews, B, Parimi, P, Kamnasaran, D. Recurrent agnathia-otocephaly caused by DNA replication slippage in PRRX1. Am J Med Genet 2013;161:803–8.
- Chassaing, N, Sorrentino, S, Davis, EE, Martin-Coignard, D, Iacovelli, A, Paznekas, W, et al. OTX2 mutations contribute to the otocephaly-dysgnathia complex. J Med Genet 2012;49:373–9.
- Sergouniotis, PI, Urquhart, JE, Williams, SG, Bhaskar, SS, Black, GC, Lovell, SC, et al. Agnathia-otocephaly complex and asymmetric velopharyngeal insufficiency due to an in-frame duplication in OTX2. J Hum Genet 2015;60:199–202.
- Rodrigyez N, Casabuenas A, Andreeva E et.al. First trimester diagnosis of agnathia-otocephaly complex: a series of 4 cases and review of the literature. J Ultrasound Med 2019;38:805-809.
- Gekas, J, Li, B, Kamnasaran, D. Current perspectives on the etiology of agnathia-otocephaly. Eur J Med Genet 2010;53:358–66.
- Donnelly, M, Todd, E, Wheeler, M, Winn, VD, Kamnasaran, D. Prenatal diagnosis and identification of heterozygous frameshift mutation in PRRX1 in an infant with agnathia-otocephaly. Prenat Diagn 2012;32:903–5.
- Sergouniotis, PI, Urquhart, JE, Williams, SG, Bhaskar, SS, Black, GC, Lovell, SC, et al. Agnathia-otocephaly complex and asymmetric velopharyngeal insufficiency due to an in-frame duplication in OTX2. J Hum Genet 2015;60:199–202.
Low set – low lying ears
Definition
- Auricle is situated low on the face
- External auditory meatus (EAM) is situated low on the face.
Etiology
There are 6 causes of “apparent” low set ears -
- Ears are truly low set without posterior rotation.
- Ears are small and appear low set.
- Ears are posteriorly rotated along their longitudinal axis and appear low set.
- Ears are over folded (lop or cup configuration) and appear low set.
- False positive – ears appear low due to fetal head position.
Ultrasound Diagnosis: There are three techniques that have been described to assess ear location, two based on the relationship between the superior auricle and outer canthi of the eyes (techniques 1 and 2), and one that is based on the location of the EAC (technique 3).
Technique 1: On a true sagittal image, draw an imaginary line between the outer canthus of the eye and the most prominent part of the occiput (occipital protuberance).
Normal: The superior attachment of the auricle should be on or above this line.
Problems associated with this technique:
1. How do you determine where the superior attachment of the auricle is, even when rotating the volume on either the x or y axis. The superior attachment of the auricle to the face is at a lower level than the location of the superior helix (Figure 25).
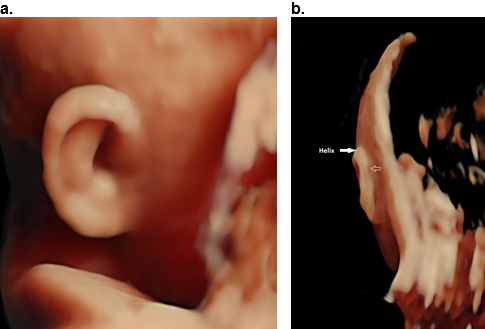
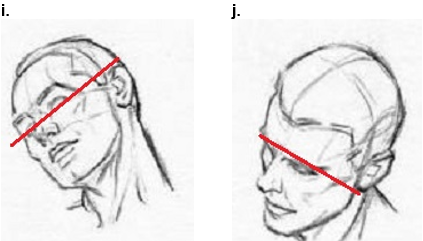
Figure 25. Determination of ear attachment.
3D renedered view in a sagittal (a) and cornal (AP) plane (b). The exact location of the attachment of the auricle to the face is not detectable in the sagittal plane and difficult to visualize on the coronal plane. The closed arrow represents the superior helix and open arrow represents the suspected level of auricle attachment.
2. The occipital protuberance cannot be visualized sonographically. So the line is not angled inferiorly (Figure 26 a, b) but is projected straight back (perpendicular) from the outer canthus of the eye (Figure 26 c,d). This line should pass through the superior helix (near the superior attachment of the auricle once the face and auricle are fully formed) (1).
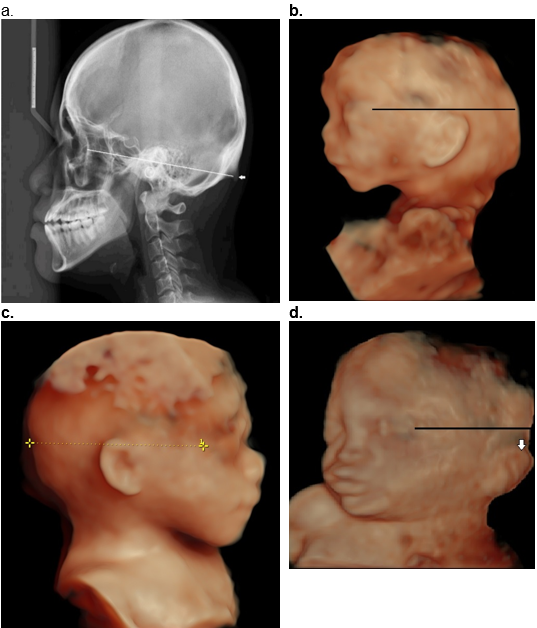
Figure 26. Technique 1 for assessment of ear location.
a. Lateral skull X-ray showing the angled line from the outer canthus of the orbit to the external occipital protuberance (EOP) (arrow).
b. The EOP cannot be visualized on ultrasound therefore the line drawn on a sagittal 3D surface rendered image of the fetus is projected straight back.
c. Line drawn perpendicular to the outer canthus of the eye passes normal below the superior helix of the outer ear.
d. Low set ears as the line passes above the superior helix of the auricle (closed arrow).
Technique 2: On a coronal plane image (AP view) draw an imaginary line through the inner and outer canthi of the eyes (the line must pass through the center of both eyes) and extend that line laterally and posteriorly. If one uses a AP technique to assess ear location, both eyes and at least one ear must be visible (Figure 27 a,b), and the volume must be manipulated to perfectly align the fetal head and face (2).
Normal: If the superior attachment of the auricle is at or above this line (normal). If the superior auricle is below this line then the ears are low set.
Problems associated with this technique:
- Both eyes and at least one ear must be visible (Figure 27 b).
- It is difficult to see both ears simultaneously on a full coronal image. By rotating the 3D image on the y-axis both ears may be seen in the same volume (Figure 27 c,d).
- The position of the subject's head relative to the observer may influence the subjective impression of the position of the ears.
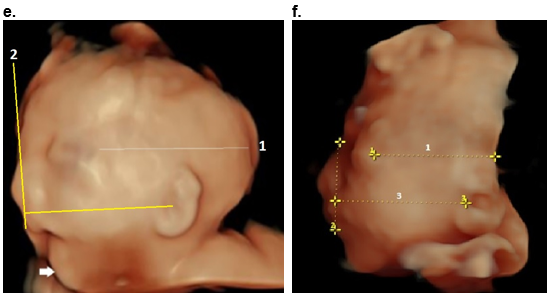
Figure 27. Technique 2 for evaluating the location of the auricle on the face.
The axis of the ear is always perpendicular to the center of the face.
a,b. Normal ear location.
-
- Line diagram. The superior portion of the helix is at or above this line (a,b).
- The drawn line is at the superior helix of the ear (closed arrow). Each ear has to be evaluated separately as both are not usually visible on the same coronal image.
c,d. Low set ears.
By rotating the image (c) on the y-axis (d) the outer canthus of the eye and full extent of the auricle is better delineated. Closed arrow – superior helix. Open arrow – lobe. * - inner and outer canthus of the eye.
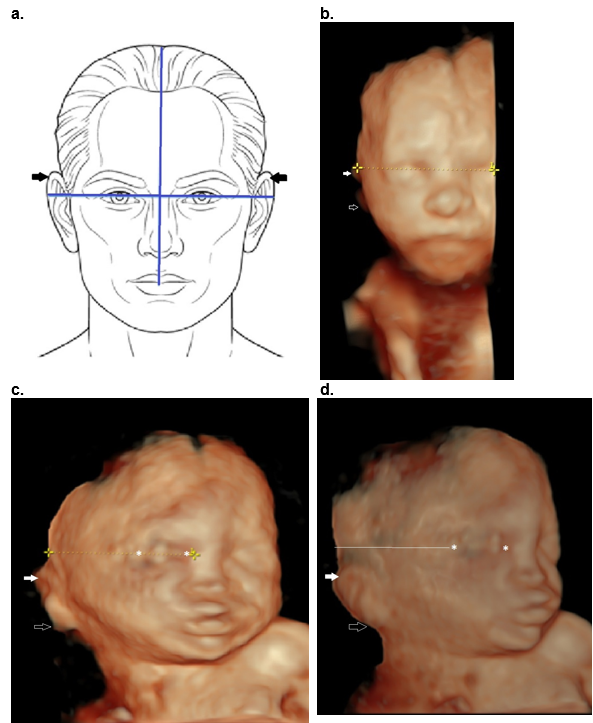
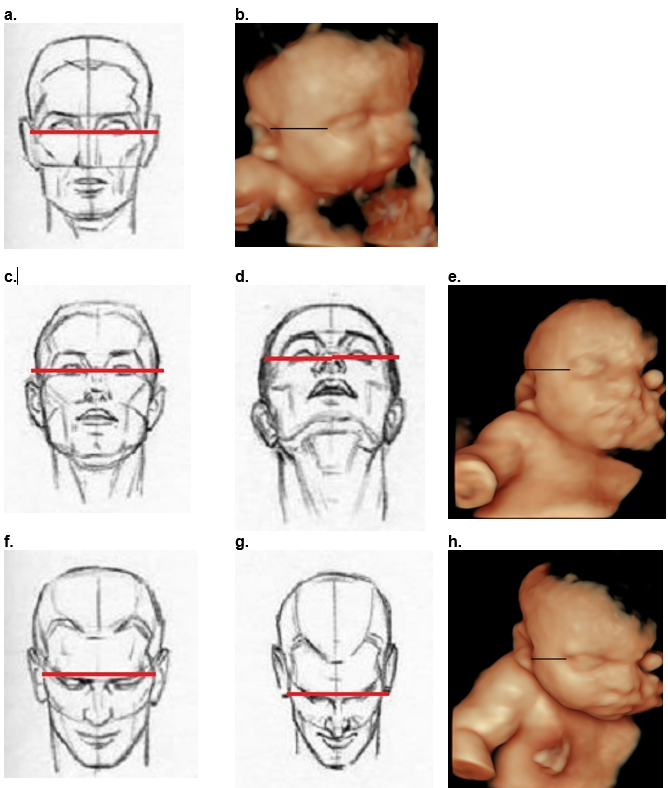
Figure 28. Ear location based on position of the fetal head. Red line represents the orbital line on the line diagram and black line represents the same line on the 3D image.
a,b. Neutral position of fetal head. Orbital line through the outer canthus of both eyes passes through the upper auricle.
c-e. When the neck is extended the fetal head looks upward and the ears project lower on the face.
f-h. When the neck is flexed the fetal head looks downward and the ears project higher on the face.
i,j. When the head is tilted to the side, the ears remain aligned with one another, but one ear is higher than the other ear.
Technique 3: Assessment of bony external auditory meatus. This was initially described by Farkas (3).
This technique evaluates the relationship of EAM to the midface and allows distinction between true low set ears and those that are posteriorly rotated, small, dysplastic and falsely appears low set.
Using this technique, you evaluate the position of the bony external auditory meatus and not the soft tissue of the ear.
Technique:
The ear and face must both be visible on the sagittal view.
Draw the profile line (connects glabella with most prominent portion of upper lip). The glabella is the smooth midline bony prominence between the supraciliary arches of the frontal bone, representing the most anterior part of the forehead.
Draw a second line from the highest portion of the EAM that perpendicularly intersects the profile line. The EAM may not be visible early in the second trimester therefore the line is drawn from the upper aspect of the concha depression (Figure 29).
Normal: The line falls above the upper edge of the alar nasi.
Abnormal: If the line falls below upper edge of alar nasi, the ear canal is low set
Problem: This is only possible to assess with 3D imaging.
This only possible if there is a visible EAM or concha depression.
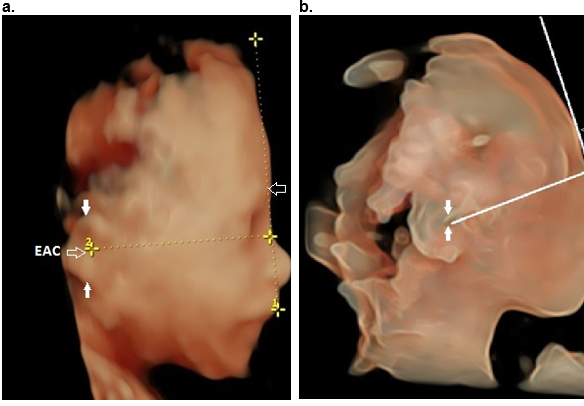
Figure 29. Ear location using technique 3.
a. Line 1 is drawn between the most prominent portion of the upper lip to the glabella (G). Line 2 is drawn perpendicular to the profile line from the highest portion of the EAM. In this normal case this line is well above the level of the ala nasi.
b. Same technique as above using silhouette mode which better delineates the EAM and concha depression (between arrows).
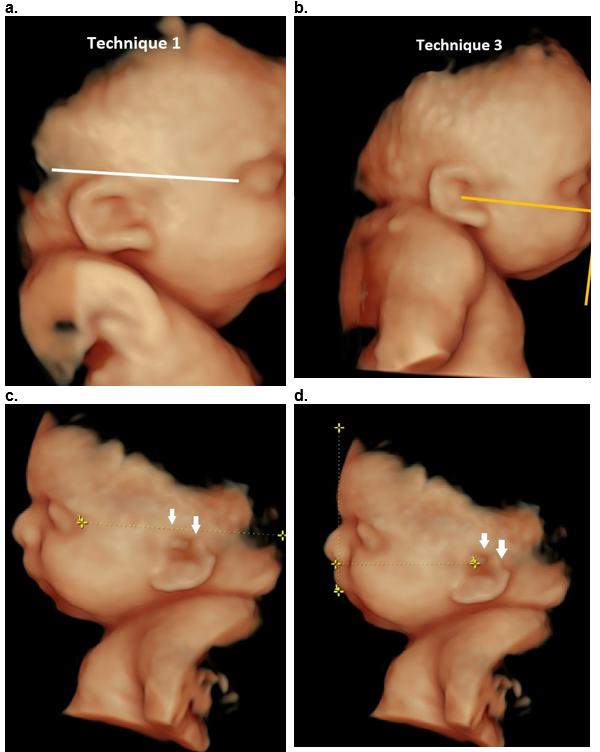
Comparison between techniques (Figure 30).
- False positive low set ears based on techniques 1 and 2 (Figure 30 a) due to posterior rotation of the ear, are shown to be normally positioned based on the location of the EAC (technique 3, Figure 30 b).
- False positive low set ears based on techniques 1 and 2 (Figure 30 c) due to a deficient superior helix of the ear are shown to be normally positioned based on the location of the EAC (technique 3, Figure 30 d).
- True low set ears based on all three techniques (Figure 30 e,f).
Figure 30. Comparison between techniques. False positive low set ears due to posterior rotation (a,b) and deficient superior helix (c,d) of the auricle. True low set ears e,f.
a,b. Comparison of techniques 1 and 3. Normal ears appear low set depending on technique. a. Posterior ear rotation gives the impression that the ears are low on technique 1. b. EAM and therefore auricle location is normally positioned when using technique 3.
c,d. CHARGE syndrome. Deficient superior helix (arrows a,b) give the impression of a low set ear (technique 1) which is shown to be normally located when using technique 3, that evaluates the location of the EAM.
e,f. True low set ears on both techniques in two different patients as the line perpendicular to the profile line is situated below the alar nasi.
Reference
- Aase IM: Microtia-clinical observations. Birth Delects Orig Artic Ser XVI 1989;(4):289.
- Porat S, Abu Zer A, Bar Lev M, Yanai N. OC11.02: Characterization of the fetal ear location and size by three dimensional ultrasound. Ultrasound Obstet Gynecol 2019;54:27-27.
- Farkas LG: Anthropometry of the Head and Face in Medicine. Raven Press, New York, 1994.
This article should be cited as Suchet I, Santos J: Abnormalities of the auricles’s position. Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, www.isuog.org, June 2023.
Leave feedback or submit an image
We rely on your feedback to update and improve VISUOG. Please use the form below to submit any comments or feedback you have on this chapter.
If you have any images that you think would make a good addition to this chapter, please also submit them below - you will be fully credited for all images used.
Feedback form
Please note that the maximum upload size is 5MB, and larger images and video clips can be sent to [email protected].