Exposure of the embryo to retinoids during the first 10 weeks may result in multiple fetal anomalies.
Acquired ear abnormalities/ facial clefts
Author: Ian Suchet1, Janelle Santos2
1. Ian Suchet MBBCh FRCPC, Calgary MFM Centre, EFW Radiology, Calgary, Alberta Canada
2. Mayo Clinic, Department of Obstetrics and Gynecology, Rochester, MN, USA
Reviewers: Karen Fung-Kee-Fung, Mauro Schenone
View the Patient Information leaflet
Acquired ear malformations
Acquired ear malformations originate from:
- Infections, especially viral infections including for rubella, cytomegalovirus, herpes simplex virus, possible for measles, mumps, hepatitis, poliomyelitis, chickenpox, Coxsackie virus, ECHO virus infections, and toxoplasmosis.
- Chemical agents, malnutrition, irradiation, Rh incompatibility, hypoxia, atmospheric pressure changes and noise exposure.
- Medicinal drugs including thalidomide, quinine and aminoglycoside antibiotics. Cytostatics and medication used in the treatment of epilepsy (e.g. diphenylhydantoin, trimethadione, and valproic acid) may also be responsible. Both excessively high doses of retinoic acid (retinoic acid embryopathy) and vitamin A deficiency (VAD syndrome) during pregnancy can produce ear malformations (1-3).
Retinoic acid embryopathy (1): Exposure of the embryo to retinoids during the first 10 wks may result in multiple fetal anomalies.
Brain malformations (70% of cases) include microcephaly, severe hydrocephalus (figure 61a), cerebellar hypoplasia, and cranial nerve defects.
Other anomalies include retrognathia, CHD, absent ossification of the parietal bones (figure 61 a,b). The skull tends to be triangular with narrowing of the frontal area and flat occiput (figure 61 g,h).
Facial nerve paralysis on the side of the more severely affected ear may be seen.
Depressed nasal bridge and midface hypoplasia may be present.
Cleft palate is found in about 15% of affected individuals (4,5), and the mandible is small in 35% (6). The eyes are occasionally microphthalmic.
Cardiac anomalies include common truncus, transposition of great vessels, atrial septal defect (ASD), VSD, tetralogy of Fallot, and aortic arch malformations. Classic DiGeorge anomaly (conotruncal malformations, thymic and parathyroid hypoplasia /aplasia) are seen in over 35% of cases (4-7). Retinal or optic nerve abnormalities are found in 20%.
Various thymic abnormalities, such as T-cell immunodeficiency and ectopic thymic tissue in the lateral neck, occur in about 35% of affected
Reported outer ear anomalies (70% of affected fetuses) include (figures 61 e-h):
- Microtia (usually asymmetrical).
- Anotia with EAC atresia.
- Low set ears.
- Slit like EAC.
The ossicles of the ears and inner ear are less frequently involved.
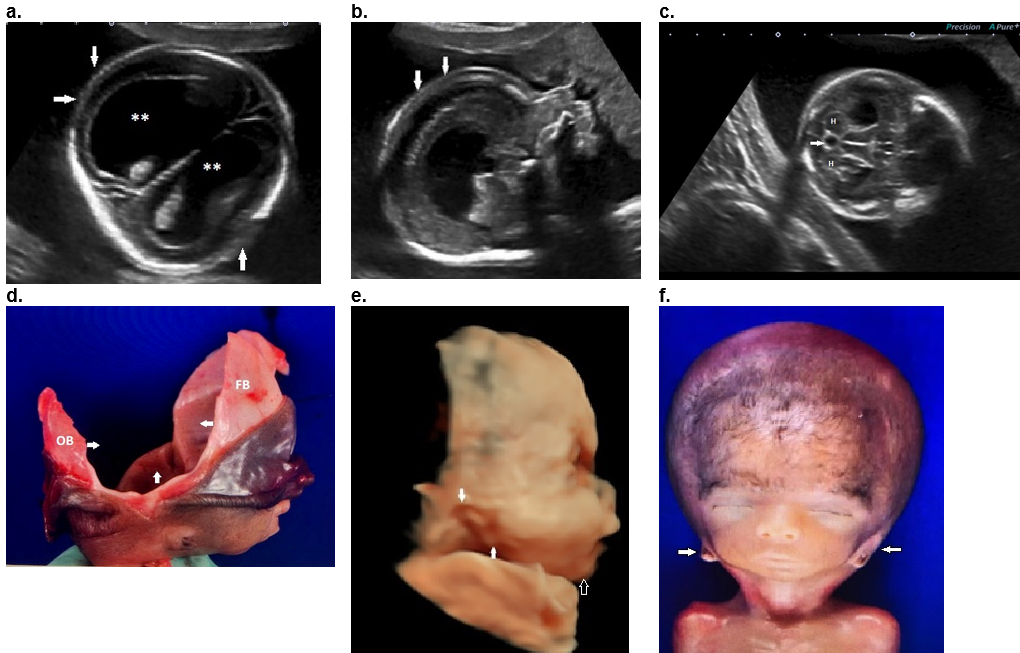
Figure 61. Retinoic acid embryopathy
a,b. Transverse and sagittal 2D images demonstrating bilateral ventriculomegaly (**) and absent ossification of the parietal bones bilaterally (arrows).
c. Hypoplastic cerebellar vermis (arrow) with normal cerebellar hemispheres (H).
d. Pathological dissection of the cranium showing complete absence of ossification in the parietal and temporal bone (between arrows) with normal frontal bone (FB) and occipital bone (OB) ossification.
e. Sagittal 3D surface rendered view of the face demonstrates small right (c) ear (type 4 microtia). The auricle of the ear is located on the chin with the long axis almost parallel to the mandible (synotia). The EAM was absent. Retrognathia (open arrow) and micrognathia were present.
f,g. Postabortal images. High triangular shaped cranium with a long flat occiput (open arrows). Both ears are low set (melotia) and located at the level of the mandible (closed arrows). Retrognathia was present.

References
- Lammer E. Preliminary observations on isotretinoin‐induced ear malformations and pattern formation of the external ear. J Craniofac Genet Dev Biol 1991 11(4): 292–295.
- Wilson RD, Johnson JA, Summers A, Wyatt P, Allen V, Gagnon A, et al Principles of human teratology: Drug, chemical, and infectious exposure J Obstet Gynaecol Can. 2007;29:911–26.
- Hersh JH. Fetal Valproate Syndrome. In: NORD Guide to Rare Disorders. Lippincott Williams & Wilkins. Philadelphia, PA. 2003:192-93’
- Lammer EJ et al: Retinoic acid embryopathy. N Engl J Med 1985;313:837-841.
- Lammer EJ et al: Isotretinoin dose and teratogenicity. Lancet 1988;2:503-504.
- Rosa RW: A syndrome of birth defects with maternal exposure to a vitamin A congener: Isotretinoin. J Clin Dysmorphol 1984;2:13-17.
- Cohen M et.al. Thymic hypoplasia associated with isotretinoin embryopathy. Am J Dis Child 1987;141:263-266.
This article should be cited as Suchet I, Santos J: Acquired ear abnormalities. Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, www.isuog.org, June 2023.
Leave feedback or submit an image
We rely on your feedback to update and improve VISUOG. Please use the form below to submit any comments or feedback you have on this chapter.
If you have any images that you think would make a good addition to this chapter, please also submit them below - you will be fully credited for all images used.
Feedback form
Please note that the maximum upload size is 5MB, and larger images and video clips can be sent to [email protected].