
Discover the latest research on screening and diagnosis of fetal anomalies: brain and heart at ISUOG 2025.
Effective screening for fetal anomalies is crucial for providing comprehensive antenatal care for women and families. Healthcare professionals involved in screening must be well-versed in current guidelines and techniques to perform their roles effectively.
Central nervous system malformations are among the most common congenital abnormalities and have profound implications for outcomes at birth. Similarly, congenital heart disease also contributes to infant morbidity and mortality. Prenatal detection of these conditions, combined with proficiency in screening techniques, enables timely patient counselling and preparation for the birth of neonates who will require specialized care and services. In some cases, prenatal diagnosis can improve birth outcomes before any intervention is necessary.
These conditions significantly impact women's health by directly influencing maternal care, pregnancy outcomes, and the overall well-being of both mother and child. Access to the latest research and advancements in prenatal diagnostics is therefore vital for improving detection rates and birth outcomes.
Prenatal detection rates can vary widely across different geographic regions, often due to differences in examiner expertise and available resources. Ensuring that healthcare providers are well-trained and equipped with up-to-date knowledge is essential for enhancing the effectiveness of fetal brain and cardiac screening.
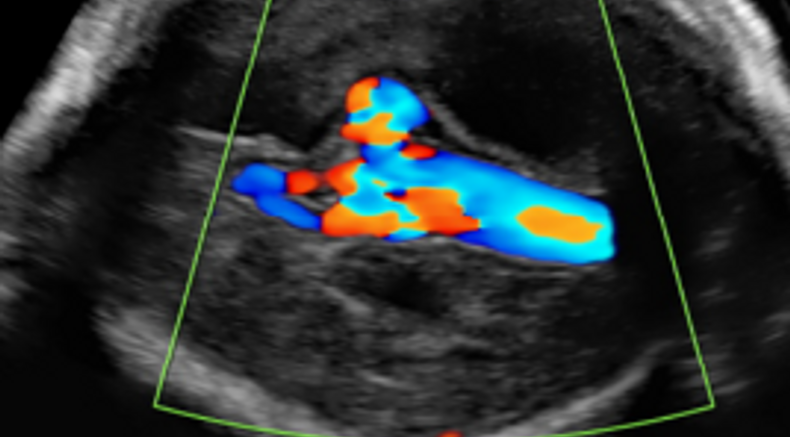
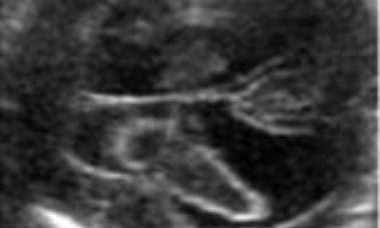
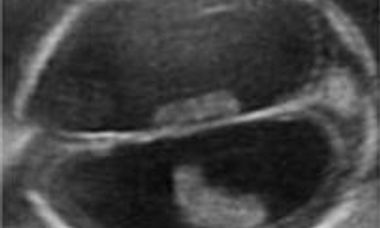
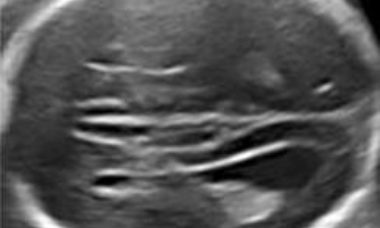
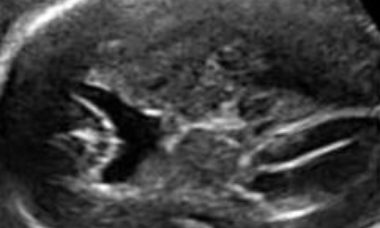
Color flow in tubular area that appeared anechoic on B-mode imaging, at midline in posterior part of base of skull
Image from: ISUOG Practice Guidelines: performance of third-trimester obstetric ultrasound scan
Why is fetal anomalies a key topic at ISUOG 2025?
Sessions where you can learn more about this topic at ISUOG 2025 World Congress
Supplement your learning Before the congress
Recent UOG articles
- Fetal corpus callosum anomalies: from disease of classification to classification of disease - L. J. Salomon, D. Paladini. First published: 19 December 2023
- ‘Choroid bar’: easy-to-seek marker of normal posterior fossa at 12–14 weeks' gestation - D. Paladini, G. Biancotto, F. Della Sala, P. V. Acharya. First published: 25 December 2023
- Enhancement of evaluation of the fetal heart as proposed by ISUOG for third trimester ultrasound examination - G. R. DeVore. First published: 17 April 2024
- Open isthmus and lambda (Λ) sign of early Joubert syndrome: elucidating development of molar tooth sign - R. K. Pooh, M. Takeda, K. Itoh, J. Yoshimatsu, K. Ogo, M. Machida, H. Ohashi, O. Shimokawa. First published: 20 April 2024
- Posterior complex: clue for suspicion of partial agenesis of corpus callosum at fetal brain screening - F. Viñals, F. Correa. First published: 30 October 2024
- Magnetic resonance imaging and tractography of sensorimotor tracts in fetuses with intraventricular hemorrhage: feasibility and added prognostic value - E. Hadi, T. Dorittke, P. Kienast, J. Binder, S. Glatter, A. Hershko-Klement, T. Lerman-Sagie, D. Prayer, G. Kasprian. First published: 15 October 2024
- Postnatal outcome of fetal cortical malformations: systematic review - N. Abadia-Cuchi, F. Felici, P. Frassanito, S. Arulkumaran, A. Familiari, B. Thilaganathan. First published: 26 September 2024
- Transvaginal SlowflowHD for embryonic and fetal hearts: human cardiac development in first trimester of pregnancy - T. Hata, R. Takayoshi, M. Sugihara, A. Koyanagi, T. Miyake. First published: 05 August 2024
- The Holy Grail of obstetric ultrasound: can artificial intelligence detect hard-to-identify fetal cardiac anomalies? - L. Drukker. First published: 01 July 2024
Lectures
Screening and diagnosis of Spina bifida 11-14 weeks - Simon Meagher
3D evaluation of the fetal CNS - Rabih Chaoui
Transposition of the great arteries - Dario Paladini
Vascular ring anomalies - Julene Carvalho
ISUOG guidelines
- Updated ISUOG Practice Guidelines: fetal cardiac screening ISUOG Practice Guidelines (updated): sonographic examination of the fetal central nervous system. Part 1: performance of screening examination and indications for targeted neurosonography
VISUOG

Abnormal 4-chamber view
Explore chapters on the abnormal 4 chamber view.
Abnormal outflow tracts
Explore chapters on aortic stenosis, common arterial trunk, fallots & variants, TGA, c-TGA, and pulmonary stenosis.
Abnormal 3-vessels view
Explore chapters on persistent left superior vena cava, aberrant right subclavian artery, double aortic arch and right aortic arch.

Holoprosencephaly
Holoprosencephaly derives from failure of separation of the cerebral hemispheres. In the most severe forms there is one undivided cerebral mass that contains a crescent shaped rudimentary ventricular cavity. In these cases, severe cranio-facial anomalies (cyclopia, hypotelorism, median cleft face) are associated.
Dandy-Walker Complex
Under this term are included a group of conditions that share in common one sonographic findings: the impression that the fourth ventricle communicates with the cisterna magna. These conditions include: Dandy-Walker malformation, Blake’s pouch cyst, vermian hypoplasia/agenesis. They have a similar sonographic appearance, particularly in early gestation, and differentiation requires a multiplanar approach.

Porencephaly
Porencephaly is characterized by single or multiple cysts replacing the brain parenchyma. The cyst may communicate with the lateral ventricle, subarachnoid space or both. It is usually a sporadic condition caused by hemorrage, ischemia or infections.
Schizencephaly
This leaflet is to help you understand what Schizencephaly is, what tests you need, and the implication of having been diagnosed with Schizencephaly for you, your baby and your family.
Intracranial Hemorrage
Intracranial hemorrage may occur within the lateral ventricles or in the subdural space. The sonographic appearance changes with time. An echogenic collection is first seen, and in the following days it develops into a complex mass frequently complicated by sever ventriculomegaly.
Severe Ventriculomegaly
The current definition is an increased size of the lateral ventricles, with a transverse diameter of the atrium in excess of 15mm without evidence of other cerebral malformations. It is a rare condition, usually a part of complex cerebral abnormalities, less frequently the consequence of obstructed cerebrospinal fluid turnover.
Agenesis of the Corpus Callosum
Agenesis of the corpus callosum may be either complete or partial. Intracranial anatomy is variable. Other intracranial anomalies are frequently encountered including ventriculomegaly, cysts, lipomas. It may be a part of genetic and genetic syndromes. The prognosis is uncertain.
Agenesis of Septum Pellucidum
Absence of the septum pellucidum is found with many cerebral malformations, including holoprosencephaly, agenesis of corpus callosum, ventriculomegaly, open spina bifida, cortical malformations. It may be an isolated abnormality and in this case the cerebral anatomy is unremarkable but for fusion of the frontal horns.
Patient information
Intracranial tumors
This leaflet is to help you understand what Intracranial tumors are, what tests you need and the implication of having been diagnosed with Intracranial tumors for you, your baby and your family.
Agenesis of the septum pellucidum
This leaflet is to help you understand what Agenesis of Septum Pellucidum is, what tests you need and the implication of having been diagnosed with Agenesis of Septum Pellucidum is for you, your baby and your family.
Ventriculomegaly
This leaflet is to help you understand what Ventriculomegaly is, what tests you need, and the implication of having been diagnosed with Ventriculomegaly for you, your baby and your family.

CME activities
- CME Activity: Workshop - Heart Beat - Normal, Irregular, Slow
- CME Activity: Workshop - Commonly Missed Cardiac Anomalies
- CME Activity: What is Wrong with this Cavum Septi Pellucidi?
- CME Activity - Fetal Neurosonography: Tips and Tricks
Questions
What are the most common abnormalities of the fetal brain and heart?
Which abnormalities of the fetal heart and brain can be diagnosed in the first trimester? Which abnormalities of the fetal brain are more commonly diagnosed in the third trimester?
How should the fetal heart be assessed in the third trimester?
What further testing should be offered when these abnormalities are encountered?