Supplement your learning for Third Trimester through Ultrasound.
Join co-Chairs Prof. Asma Khalil and Prof. Alexandros Sotiriadis for this engaging and informative course. Together with assistance from the authors of the new ISUOG guidelines they will dive into guideline to share with you practical and theoretical understanding of the third trimester through ultrasound. This course offers attendees a valuable opportunity to gain a comprehensive understanding of the new guidelines and learn how to apply them in practical situations.
Learning Objectives:
- Understand the overall rationale behind conducting a third-trimester scan.
- Demonstrate proficiency in the technique of performing a third-trimester ultrasound scan.
- Analyse the rationale and morphology of structural elements of the fetus that can be examined during the third trimester.
- Comprehensively assess fetal growth, including the methods and timing involved.
- Apply effective screening methods and management strategies for abnormal fetal growth.
- Perform a late assessment of the placenta and umbilical cord during the third trimester.
- Learn how to implement an algorithm for the assessment of amniotic fluid in the third trimester.
- Understand the rationale for Doppler assessment in low-risk pregnancies during the third trimester.
Explore the topic before you attend our course
In order to make the most of this learning experience and help you achieve your learning objectives, we have prepared a path to guide you from the essentials to our course’s topics through ISUOG resources. The material below, will take you from the most basics to a more comprehensive view of Third Trimester through Ultrasound, some open to everyone and some available only to ISUOG members –some may even grant you CME points:
Some of these activities are exclusively available to our members. Become a member today.
VISUOG chapters
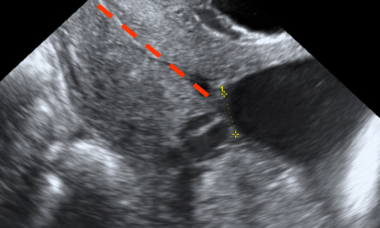
Vasa Previa
Vasa previa is a rare condition (in 1300 to 1 in 2500 deliveries) that can result in perinatal mortality at rupture of fetal membranes.
Placenta Previa
Placenta previa is diagnosed when the placenta overlies or is close to the internal cervical os, obstructing delivery. The incidence is of 5 in 1000 deliveries and it has recently increased due to the rise in cesarean deliveries. PP is associated with a higher risk of adverse maternal outcomes.

Placenta Accreta Spectrum Disorders: Abnormally Adherent and Invasive Placenta
The placenta accreta spectrum disorders include both abnormally adherent and invasive placenta. Targeted screening is essential for these disorders due to the association between low-lying or previa placenta and previous cesarean delivery. Prenatal diagnosis is possible by ultrasound.
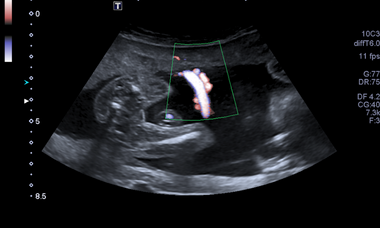
Velamentous Cord Insertion
Velamentous cord insertion occurs when the placental end of the umbilical cord contains divergent vessels that are surrounded by membranes and are not supported by Whartons Jelly.
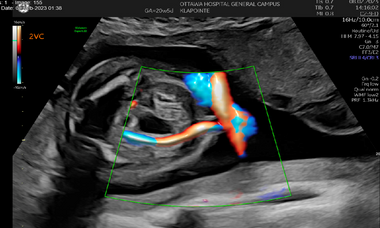
Vascular Abnormalities of the Umbilical Cord
Abnormalities of the umbilical vessels discussed in this chapter include aberrations in numbers of vessels and select structural variations such as umbilical vein varices.

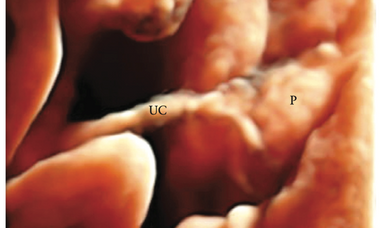
Angiomyxoma of Umbilical Cord
Angiomyxoma of the umbilical cord is a rare tumor that can be detected by Ultrasound prenatally as a complex solid-cystic mass.

Placental Lakes
Placental lakes or placental lacunae are well-demarcated, mainly sonolucent avillous spaces of diverse size and shape, surrounded by placental tissue with normal echogenicity /subchorionic location. Their etiology is varied, so the contents of the lacunae can vary, with many containing venous maternal blood.
Placental Masses, Variants, and Placental Lesions
Placental cysts are non-vascular lesions that may occur within the body, or on the surface of the placenta.

Placental Diseases
The purpose of this chapter is to be able to address three placental pathologies that cause controversy among both imaging specialists and obstetricians: 1) placental hematomas, 2) massive perivillous fibrin deposition (MPFD), and 3) placental infarcts.

Doppler Assessment of the Fetal Cerebral Circulation
Evaluation of cerebral circulation in the fetus has long been used for clinical guidance in growth restriction and those at risk for fetal anemia.
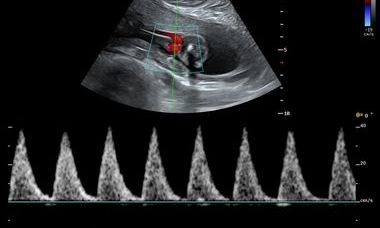
Umbilical Artery Doppler
Doppler assessment of the placental circulation plays an important role in screening for impaired placentation and its complications of pre-eclampsia, fetal growth restriction (FGR), and perinatal death.
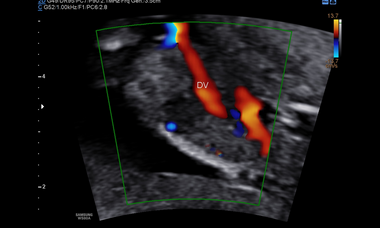
Ductus venosus
The ductus venosus is an important regulator of fetal circulation as it shunts oxygenated blood from the umbilical vein directly into the inferior vena cava.
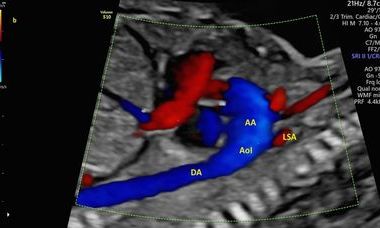
Aortic Isthmus
The aortic isthmus (AoI) is an aortic segment located between the origin of the left subclavian artery and the junction of the ductus arteriosus to the descending aorta.
Small for gestational age (SGA) and fetal growth restriction (FGR)
A fetus is considered to be small for gestational age (SGA) when its size falls below a predefined threshold for its gestational age. The most common definition of SGA is estimated fetal weight (EFW) or abdominal circumference (AC) below the 10th percentile of given reference ranges.
UOG Articles
M. van Roekel, J. Henrichs, A. Franx, C. J. Verhoeven, A. de Jonge
27 January 2023
N. Fratelli, F. Prefumo, C. Maggi, C. Cavalli, A. Sciarrone, A. Garofalo, E. Viora, P. Vergani, S. Ornaghi, M. Betti, I. Vaglio Tessitore, A. F. Cavaliere, S. Buongiorno, A. Vidiri, E. Fabbri, E. Ferrazzi, V. Maggi, I. Cetin, T. Frusca, T. Ghi, C. Kaihura, E. Di Pasquo, T. Stampalija, C. Belcaro, M. Quadrifoglio, M. Veneziano, F. Mecacci, S. Simeone, A. Locatelli, S. Consonni, N. Chianchiano, F. Labate, A. Cromi, E. Bertucci, F. Facchinetti, A. Fichera, D. Granata, F. D'Antonio, F. Foti, L. Avagliano, G. P. Bulfamante, G. Calì, the ADoPAD (Antenatal Diagnosis of Placental Adhesion Disorders) Working Group
05 March 2022
W. Zhang, S. Geris, N. Al-Emara, G. Ramadan, A. Sotiriadis, R. Akolekar
31 July 2020
A. Ficara, A. Syngelaki, A. Hammami, R. Akolekar, K. H. Nicolaides
08 October 2019
Routine ultrasound at 32 vs 36 weeks’ gestation: prediction of small-for-gestational-age neonates
A. Ciobanu, N. Khan, A. Syngelaki, R. Akolekar, K. H. Nicolaides
18 March 2019
Performance of third-trimester combined screening model for prediction of adverse perinatal outcome
J. Miranda, S. Triunfo, M. Rodriguez-Lopez, M. Sairanen, H. Kouru, M. Parra-Saavedra, F. Crovetto, F. Figueras, F. Crispi, E. Gratacós
05 October 2016
Learning Modules
View lectures on similar subjects.
CNS anomalies in the third trimester: a diagnostic and counselling challenge
D.Prayer, G. Malinger, K.Haratz 2022
Vasa previa: high time to screen
C. Lees, A.Odibo, D. Srinivasan Y. Oyelese 2022
Scan demonstration: Accreta for beginners
B.Thilaganathan 2021
Should all women have third trimester ultrasound screening
A. Odibo 2019
Late FGR and stillbirth: how strong is the relationship?
L.Poon 2019
Why a third trimester Randomised Controlled Trial is needed
C. Lees 2017